


Internal Anatomy of the Pulp System: Clinical Relevance and Determination
Internal Anatomy of Pulp System
Understanding the internal anatomy of the pulp is fundamental in endodontics. In fact, lack of knowledge about pulp morphology is considered the second most common cause of treatment failure, following only diagnostic and treatment planning errors. For successful outcomes, clinicians must master the normal configuration of the pulp and its possible variations, while applying special techniques to explore and treat the internal anatomy effectively.
Methods for Determining Pulp Anatomy
1. Textbook Knowledge
- Textbooks remain the most reliable foundation.
- Students must memorize the following for each tooth:
➔ Number of roots.
➔ Number and position of canals.
➔ Cross-sectional and longitudinal shapes.
➔ Common curvatures (particularly in the faciolingual plane).
➔ Root outlines in all dimensions. - Approximate percentages and diagrams of variations are particularly useful.
2. Radiographic Evidence
- Conventional periapical radiographs are helpful but have limitations:
➔ They provide only two dimensions, often missing the third.
➔ Canals appear deceptively uniform and tapered, whereas in reality they may show significant irregularities. - Special radiographic techniques (angled views, advanced imaging) improve detection of:
✔ Missed canals.
✔ Root curvature and anomalies.
3. Exploration During Treatment
- Additional insights are obtained during:
➔ Access cavity preparation.
➔ Canal exploration with instruments. - Limitation: canals may still be difficult to locate or may remain hidden despite exploration.
Summary Table: Approaches to Determining Pulp Anatomy
| Method | Advantages | Limitations |
|---|---|---|
| Textbook Knowledge | Provides baseline, common variations, percentages | Cannot account for all patient-specific anatomy |
| Radiographs | Visualizes roots and canals, detects curvatures | Only 2D; may miss hidden or extra canals |
| Exploration | Real-time confirmation during access | Some canals remain hard to detect |
General Considerations in Root and Canal Anatomy
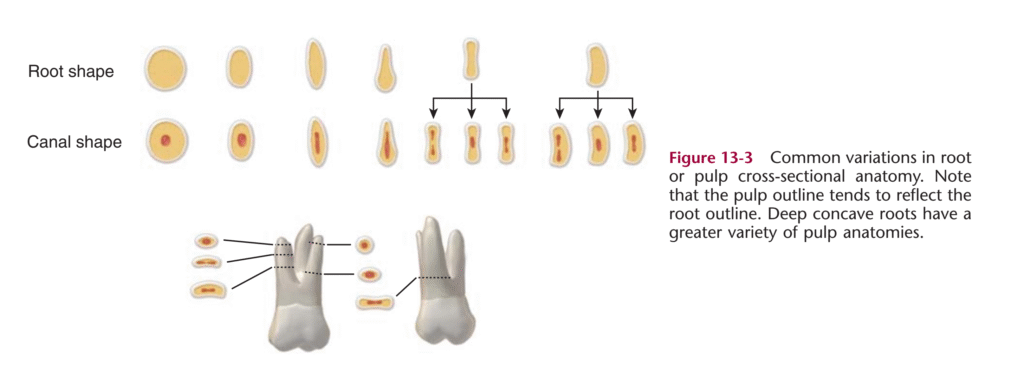
- Key principle: the pulp system mirrors the external tooth shape.
- Root cross-sections can vary significantly and commonly include seven patterns:
- Round
- Oval
- Long oval
- Bowling-pin
- Kidney-bean
- Ribbon
- Hourglass
✦ A single root may show different cross-sectional shapes at different thirds (cervical, middle, apical).
✦ Importantly, a canal is rarely perfectly round—assuming so may lead to improper canal preparation.
Canal Morphology and Variations
- Root canals may:
➔ Branch, divide, and rejoin before reaching the apex. - Vertucci’s classification describes eight canal configurations, which remains the standard reference.
- Gender and ethnicity influence variations:
✔ Example: Mandibular premolars in African-American patients show extra canals more frequently (33% of first premolars, 8% of second premolars) compared to Caucasian patients (14% and 3%, respectively).
Clinical Tip: Always consider patient background and tooth group when predicting root canal anatomy.

Identification of Canals and Orifices
To clean, shape, and obturate a canal, it must first be accurately located.
- Rule of thumb: assume the presence of two canals until proven otherwise.
- Exceptions (rarely two canals):
- Maxillary anterior roots.
- Premolars with two or three roots.
- Distobuccal and lingual roots of maxillary molars.
- All other maxillary and mandibular roots demand thorough searching for additional canals.
Laws of Location of Canal Orifices
The pulp chamber floor and walls provide valuable guidance. According to Krasner and Rankow, six fundamental “laws” help identify orifices:
- Symmetry 1: Canal orifices are equidistant from a mesiodistal line through the pulp chamber floor (exception: maxillary molars).
- Symmetry 2: Canal orifices lie on a line perpendicular to the mesiodistal line across the chamber floor (exception: maxillary molars).
- Orifices’ Location 1: Found at the junction of walls and floor.
- Orifices’ Location 2: Located at line angles of the floor-wall junction.
- Orifices’ Location 3: Found at the terminus of root developmental fusion lines.
- Color Change Law: The pulp chamber floor is always darker than the surrounding walls.
Clinical Example
A 45-year-old patient presents for endodontic therapy on a mandibular first molar.
- Standard periapical radiograph shows only two visible canals.
- Following the laws of symmetry and color change, a third canal (MB2) is identified during access preparation.
- Failure to detect this canal could have resulted in persistent symptoms and eventual treatment failure.
Components of the Pulp System
The pulp cavity is composed of two main portions:
- Coronal portion → the pulp chamber.
- Radicular portion → the root canal.
Additional features include:
✦ Pulp horns
✦ Canal orifices
✦ Accessory (lateral) canals
✦ Apical foramen
The internal anatomy of these structures changes over time due to the deposition of secondary dentin and cementum.
Pulp Horns
- Represent areas that clinicians avoid in restorative procedures, but target during access preparation.
- Typically:
➔ One pulp horn per cusp in posterior teeth.
➔ Mesial and distal horns in incisors. - Age-related changes:
- In young teeth → pulp horns extend near the height of contour.
- In older teeth → secondary dentin formation moves them closer to the cervical margin.
- Clinical tip: During access preparation, measure from the occlusal surface or cusp tip to the pulp horn/chamber roof using a bur and handpiece.
Pulp Chamber
- Located in the center of the crown and the trunk of the root.
- Shape depends on:
✦ Crown and root morphology
✦ Tooth age
✦ History of irritation - In mature molars, the roof of the chamber lies approximately at the cementoenamel junction (CEJ).
Root Canals
- Extend from a funneled orifice to the apical foramen.
- Most canals are curved, often in the faciolingual plane.
➔ This curvature is often invisible on radiographs.
➔ Assuming straightness may lead to over-enlargement, ledging, or perforation. - Rule of thumb: Always assume a canal is curved.
Variations in Canal Shape
- Influenced by root size, degree of curvature, age, and pathology.
- When two canals exist in one root → they tend to be more oval.
- Shapes include:
✔ Bowling pin
✔ Kidney bean
✔ Hourglass
✔ Ribbon - Shape progression in one root:
- Cervical third → may appear round or irregular.
- Middle third → often deep oval.
- Apical third → tends to be oval or flattened.
Clinical Note
Irregularities such as isthmuses, fins, cul-de-sacs, and intercanal communications are common in posterior teeth. These areas are:
✦ Difficult to access with instruments/irrigants.
✦ Rarely obturated completely.
Accessory (Lateral) Canals
- Lateral branches that connect the main canal with the periodontium.
- Contain connective tissue and vessels.
- Location: can appear at any level, but are more common in:
➔ Apical third
➔ Posterior teeth - Clinical significance:
- They allow passage of irritants from the pulp to the periodontium.
- Rarely cleaned or shaped effectively.
- Occasionally filled with obturating material, but not essential for treatment success.
Apical Region
Development
- The apex is the terminal portion of the root.
- In young teeth → relatively straight.
- With age → curves distally due to continued cementum deposition and tooth eruption.
- Alterations can also result from resorption or irregular cementum apposition.
- Anatomy becomes nonuniform and unpredictable.
Apical Foramen
- Its size and configuration vary with maturity.
- In immature teeth → wide open.
- With age → narrows due to dentin and cementum deposition.
- Usually does not coincide with the anatomic root apex, but is offset by 0.5–1.0 mm.
- Not visible on radiographs → clinicians rely on average values or electronic apex locators.
Variations in Apical Anatomy
- Apical canal system is often complex:
✔ Twists and turns
✔ Division into deltas with multiple ramifications
✔ Long oval or ribbon-shaped canals (not round) - Non-round canals cannot be enlarged to round shapes without risking perforation or root weakening.
Apical Constriction
- Its presence is unpredictable.
- The cementodentinal junction (CDJ) was once believed to define the constriction, but this is not reliable.
- It is not visible radiographically and usually not detectable even by experienced clinicians.
MCQs in Internal Anatomy of the Pulp System
📊 Summary Table – Key Features of Pulp System Components
| Component | Location/Description | Clinical Relevance |
|---|---|---|
| Pulp Horns | Associated with cusps (posterior) or mesial/distal (incisors). | Important for access preparation; position shifts with age. |
| Pulp Chamber | Central crown/trunk; roof at CEJ in mature molars. | Shape reflects crown/root morphology. |
| Root Canals | Extend root length; mostly curved (faciolingual). | Must assume curvature; irregularities complicate cleaning/obturating. |
| Accessory Canals | Lateral branches, common in apical third/posteriors. | Allow irritant passage; not critical to obturation success. |
| Apical Foramen | Slightly offset from anatomic apex; size reduces with age. | Guides extent of cleaning/obturation (short of apex). |
| Apical Variations | Delta systems, twists, oval canals. | Hard to detect, clean, or fill completely. |
| Apical Constriction | Often absent/unpredictable. | CDJ unreliable; not visible radiographically. |
Variations of Root and Pulp Anatomy
Understanding the diversity of root and pulp anatomy is essential for successful endodontic and restorative procedures. While most teeth follow predictable patterns, numerous morphological variations exist that can complicate diagnosis, access preparation, and treatment.
1. General Considerations
- Variations are most common in:
✦ Maxillary lateral incisors
✦ Maxillary and mandibular premolars
✦ Maxillary molars - Root anomalies are frequently bilateral.
- Careful radiographic evaluation and clinical awareness are crucial before initiating treatment.
2. Common Variations and Abnormalities
Dens Invaginatus (Dens in Dente)
- Definition: Infolding of the enamel organ during morphodifferentiation.
- Most common in: Maxillary lateral incisors.
- Clinical significance:
- Early pulp–oral cavity communication → often requires root canal treatment.
- Severity varies; severe cases may need surgical intervention.
- Prognosis often questionable.
- Diagnosis: Visible radiographically, but small/obscure cases may be missed.
- Minor form: Lingual pit on maxillary anterior teeth.
Dens Evaginatus
- Definition: A tubercle-like bulge on the occlusal surface.
- Most common in: Mandibular premolars.
- Prevalence: Higher in Asian, Native American, and Hispanic populations.
- Clinical concern:
- Tubercle often contains pulp extension.
- Fracture → direct pulp exposure → necrosis → apexification required.
- Preventive management:
- Early removal of the tubercle using a bur.
- Pulp capping + durable sealing restoration (e.g., amalgam).
High Pulp Horns
- Pulp horns extending deep into cusp regions.
- May cause premature exposure:
- By dental caries.
- During cavity preparation.
- Common site: Mesiobuccal cusp of first molars.
- Usually not detectable radiographically.
Lingual Groove
- Site: Typically maxillary lateral incisors.
- Description: Infolding of dentin running from cervical to apical direction.
- Complication:
- Creates a narrow periodontal defect.
- May connect with pulp → combined endodontic/periodontal lesion.
- Prognosis: Poor; treatment unpredictable. Extraction often required.
Dilaceration
- Definition: Severe/complex curvature of a root.
- Causes:
- Deflection of epithelial diaphragm by anatomical structures (e.g., sinus wall, mandibular canal).
- Note:
- Common in faciolingual plane.
- May not be evident on standard radiographs.
3. Other Notable Variations
| Variation | Common Site | Clinical Challenge | Prognosis |
|---|---|---|---|
| C-shaped canal | Mandibular second molars (esp. Asian patients) | Complex internal anatomy → difficult cleaning/obturation | Questionable |
| Three-rooted maxillary premolar | Maxillary premolars | Unusual chamber and root configuration | Challenging |
| Distolingual third root | Mandibular first molars | Can occur in all races | May require referral |
4. Modern Diagnostic Aids
- Cone-beam CT (CBCT): Provides detailed 3D images of tooth/root anatomy.
- Micro-CT research: Offers advanced morphologic data but not yet feasible for routine clinical use.