
Clinical Examination of the Edentulous Patient (Complete Denture) _ Intraoral examination
Clinical Examination of the Edentulous Patient (Complete Denture) _ Intraoral examination
Clinical Examination of the Edentulous Patient (Complete Denture) _ Intraoral examination
Intraoral Examination for Complete Denture Fabrication
Following the extraoral assessment, a meticulous intraoral examination is critical for diagnosing the patient’s condition and formulating an effective treatment plan for complete dentures. This examination evaluates the health and characteristics of the oral tissues and anatomical structures that will support, retain, and stabilize the prosthesis.
1. Oral Mucosa
The mucosa covering the edentulous ridges must be thoroughly evaluated for color, condition, and thickness, as these factors directly impact denture comfort and stability.
- Color: Healthy mucosa typically exhibits a uniform pink color. Erythema (redness) signals inflammation, which may be caused by an ill-fitting denture, local infection, smoking, or systemic disease. Inflamed tissues are unsuitable for accurate impression making. Other discolorations, such as white patches (e.g., frictional keratosis), should be noted and investigated.
- Condition (House’s Classification):
- Class I: Healthy mucosa.
- Class II: Irritated mucosa.
- Class III: Pathologic mucosa.
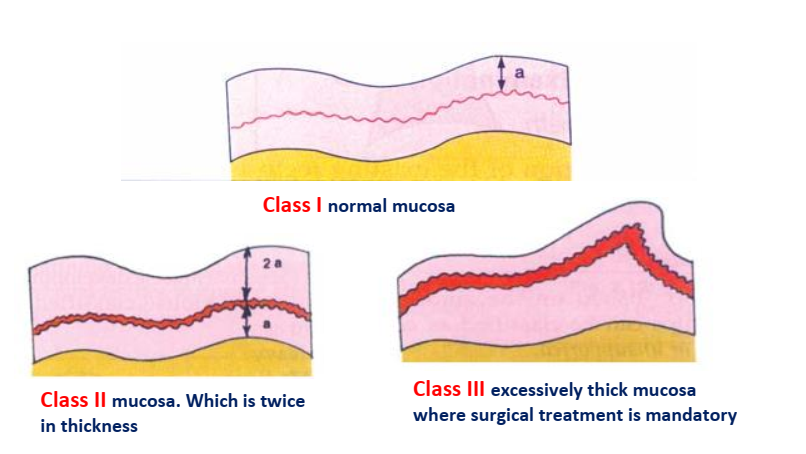
- Thickness and Quality (House’s Classification): The consistency of the mucoperiosteum is crucial for equalizing pressure under the denture base.
- Class I: Normal, uniform density (approximately 1 mm thick). The tissue is firm and provides an ideal cushion for the denture base.
- Class II: Can be of two types: (a) Thin investing membrane, highly susceptible to irritation, or (b) Mucous membranes twice the normal thickness.
- Class III: Excessively thick investing membranes with redundant tissue, often requiring pre-prosthetic treatment.
2. Saliva
The quality and quantity of saliva are vital for denture retention through cohesive and adhesive properties.
- Class I: Normal quality and quantity. Ideal for denture retention.
- Class II: Excessive saliva (sialorrhea), often mucinous, which can complicate clinical procedures.
- Class III: Xerostomia (dry mouth). The remaining saliva is often thick and mucinous. Xerostomia leads to poor retention and tissue irritation, while excessive salivation can disrupt the denture seal.
3. Residual Alveolar Ridge
The morphology of the edentulous ridges is a primary determinant of denture support, retention, and stability.
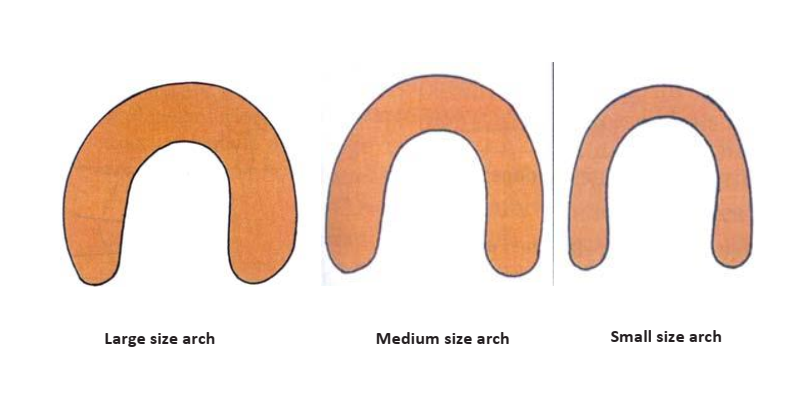
- Arch Size: The denture-bearing area increases with arch size, enhancing retention. A significant discrepancy between maxillary and mandibular arch sizes can complicate teeth arrangement and compromise stability on the smaller arch.
- Class I: Large arch (ideal for retention and stability).
- Class II: Medium arch (good retention and stability).
- Class III: Small arch (difficult to achieve good retention and stability).
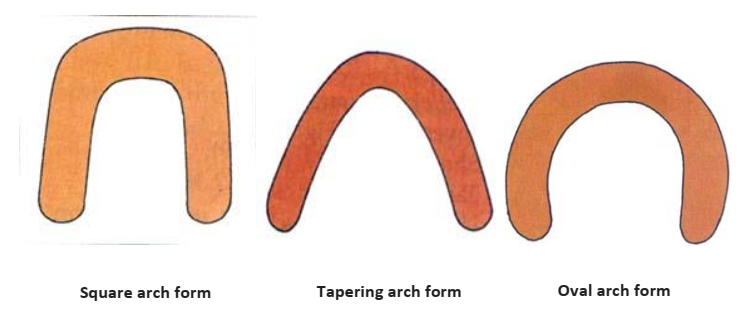
- Arch Form: Influences denture support and tooth selection. Forms include square, ovoid, and tapered. Discrepancies between arches can create challenges in teeth arrangement.
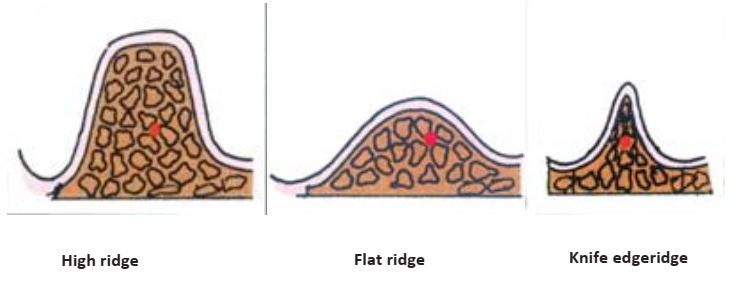
- Ridge Contour: Assessed by inspection and palpation to detect bony spicules. Ideal ridges offer a broad, flat crest for support.
- Primary Classification:
- High ridge with a flat crest and parallel sides (most ideal).
- Flat ridge.
- Knife-edged ridge.
- Primary Classification:
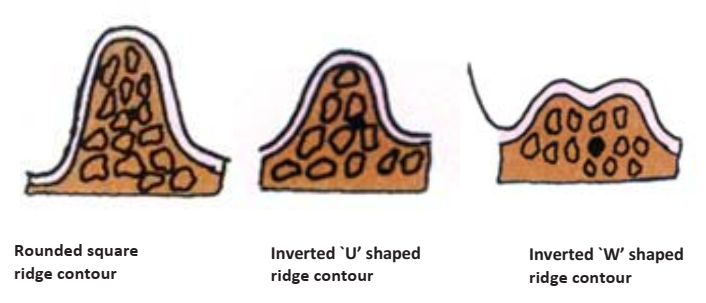
- Maxillary Ridge Classification:
- Class I: Square to gently rounded.
- Class II: Tapering or ‘V’ shaped.
- Class III: Flat.
- Mandibular Ridge Classification:
- Class I: Inverted ‘U’ shape (parallel walls, broad crest).
- Class II: Inverted ‘U’ shape (short with flat crest).
- Class III: Unfavourable (e.g., Inverted ‘W’, inverted ‘V’, or undercut ridges “results due to labioversion or linguoversion of the teeth”).
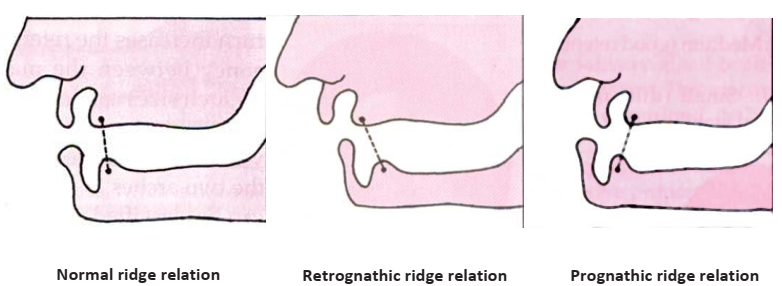
- Ridge Relation: The anteroposterior relationship between the maxillary and mandibular ridges (Angle’s Classification).
- Class I: Normal.
- Class II: Retrognathic.
- Class III: Prognathic.
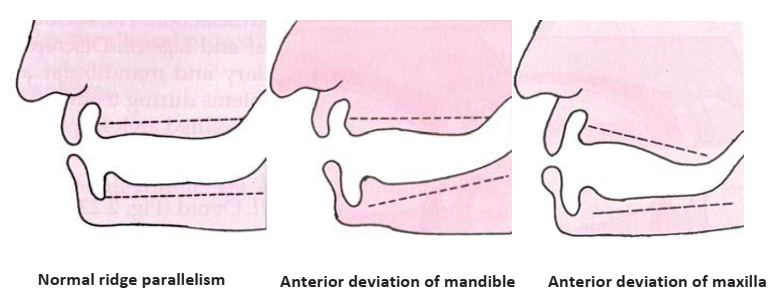
- Ridge Parallelism: Refers to the parallelism of the ridge planes to the occlusal plane. Parallel ridges simplify teeth arrangement.
- Class I: Both ridges are parallel to the occlusal plane.
- Class II: The mandibular ridge diverges anteriorly.
- Class III: The maxillary ridge or both ridges diverge anteriorly.
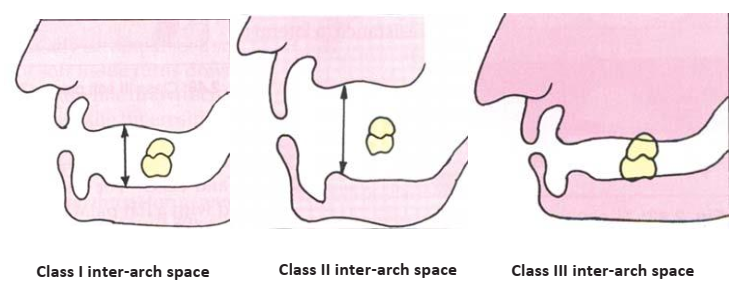
- Inter-Arch Space: The space available for artificial teeth.
- Class I: Ideal space.
- Class II: Excessive space, often due to ridge resorption, leading to decreased retention.
- Class III: Insufficient space, making teeth arrangement difficult but potentially increasing stability by reducing leverage.
4. Palate
The anatomy of the hard and soft palate significantly affects denture retention and border sealing.
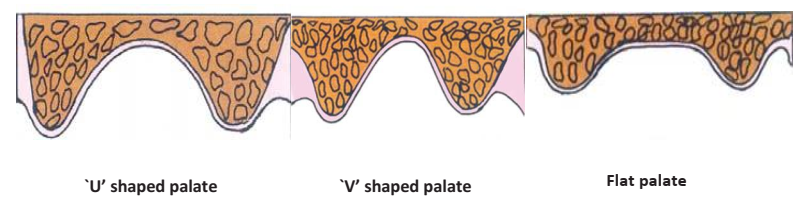
- Hard Palatal Vault Form:
- U-shaped: Ideal for retention and stability.
- V-shaped: Retention is compromised as the peripheral seal is easily broken.
- Flat: Offers reduced resistance to lateral forces.
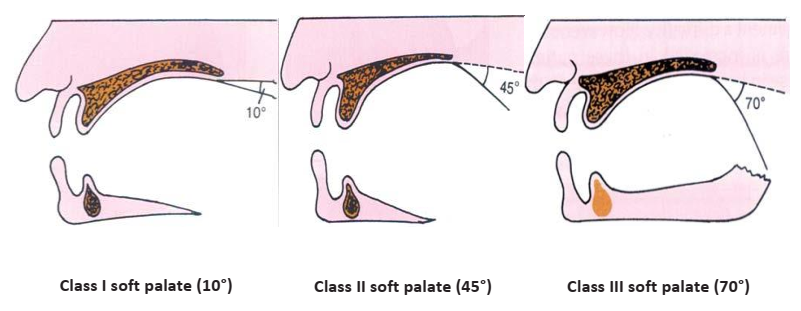
- Soft Palate and Palatal Throat Form: The angle and mobility of the soft palate determine the extent of the posterior palatal seal.
- Class I: Horizontal soft palate with minimal movement (allows for maximum tissue coverage for the seal).
- Class II: Soft palate at a 45° angle to the hard palate.
- Class III: Soft palate at a 70° angle (allows for minimal tissue coverage for the seal). Often associated with a V-shaped vault.
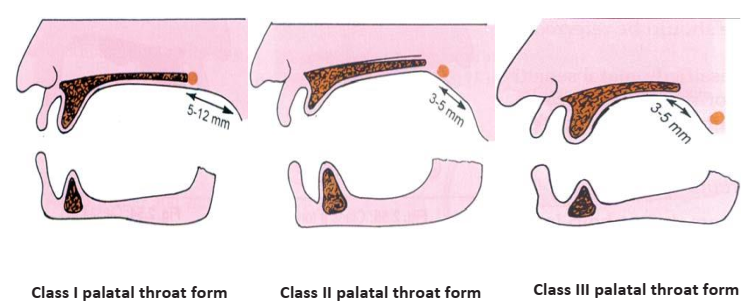
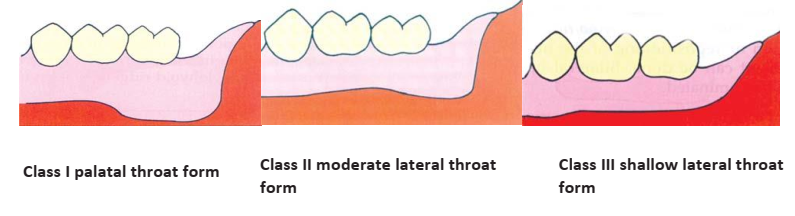
- Lateral Throat Form (Retromylohyoid Fossa): Classified by Neil as Class I (deep), Class II (moderate), or Class III (shallow), influencing the lingual flange extension of the mandibular denture.
- Gag Reflex and Palatal Sensitivity: An exaggerated gag reflex must be managed. House classified sensitivity as Class I (Normal), Class II (Hyposensitive), or Class III (Hypersensitive).
5. Anatomical Variations and Obstacles
- Bony Undercuts: Interfere with the path of insertion and peripheral seal. Common in the maxillary anterior and tuberosity regions, and under the mandibular mylohyoid ridge. Surgical reduction may be necessary.
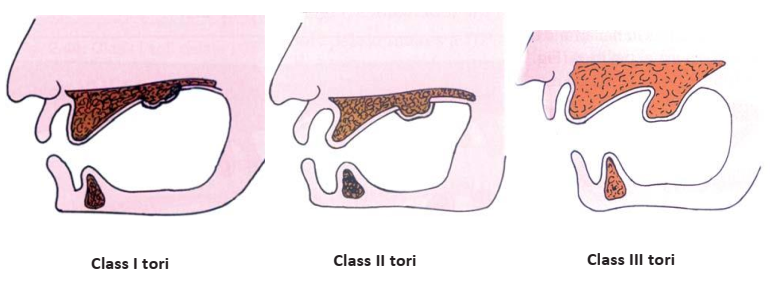
- Tori: Bony exostoses on the palate (torus palatinus) or the lingual aspect of the mandible (torus mandibularis).
- Class I: Absent or minimal, non-interfering.
- Class II: Moderate size, may require denture relief but not surgery.
- Class III: Large, compromising denture function and fabrication, typically requiring surgical removal.
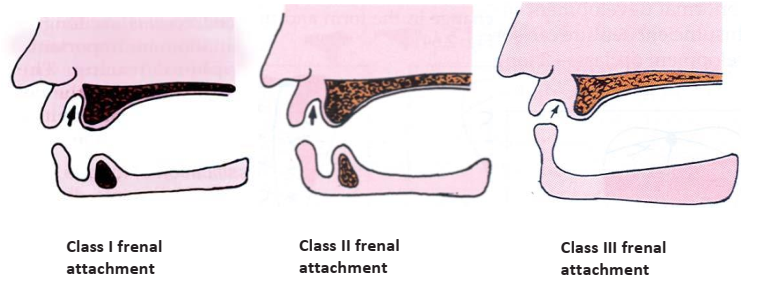
- Muscle and Frenal Attachments: The position relative to the ridge crest is critical. Attachments near the crest can dislodge the denture during function.
- Border Attachments (House): Class I (>0.5 inches from crest), Class II (0.25-0.5 inches), Class III (<0.25 inches, often requiring surgical correction).
- Frenal Attachments (House): Class I (away from crest), Class II (near crest), Class III (encroaching on the crest, may require surgery).

6. Tongue and Floor of the Mouth
- Tongue:
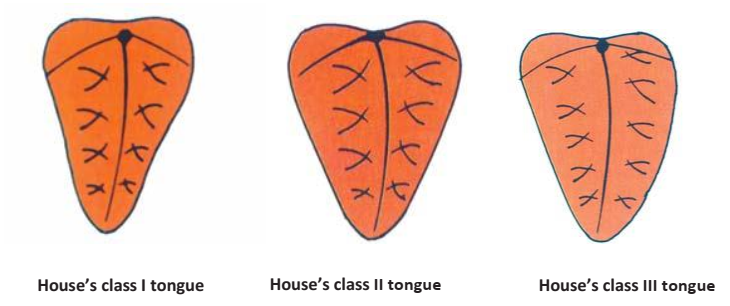
- Size (House’s Classification): A large tongue (Class III) can compromise stability; a small tongue may not aid in seal formation.
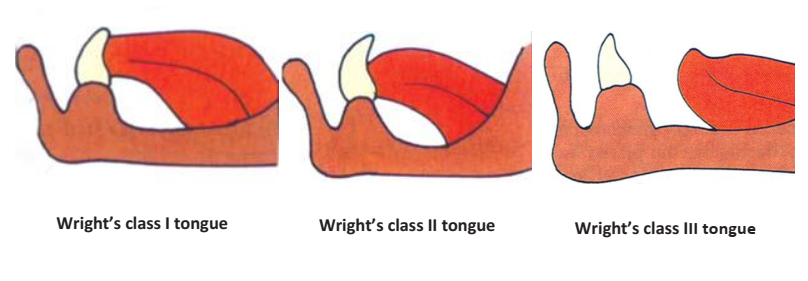
- Position (Wright’s Classification):
- Class I: Ideal position in the floor of the mouth, facilitating a good lingual seal.
- Class II: Flattened and broadened.
- Class III: Retracted and depressed, making it challenging to establish a peripheral seal without denture displacement.
- Floor of the Mouth: The resting and active height of the floor of the mouth determines the length of the lingual flange. A high floor of the mouth (close to the ridge) limits flange extension and retention. Measurement is taken with the tongue elevated to simulate functional movement.



