ANATOMY OF THE PULP CAVITY AND ROOT CANAL (Endodontics MCQs)
ANATOMY OF THE PULP CAVITY AND ROOT CANAL - Endodontics MCQs
ANATOMY OF THE PULP CAVITY AND ROOT CANAL – Endodontics MCQs
ANATOMY OF THE PULP CAVITY AND ROOT CANAL – Endodontics MCQs
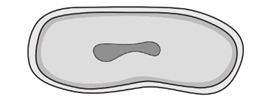
1. Cervical cross-section of maxillary first premolar has:
A. A round shape
B. Elliptical shape
C. Oval shape
D. Square shape
2. Of the following permanent teeth, which is least likely to have two roots?
A. Maxillary canine
B. Mandibular canine
C. Maxillary first premolar
D. Mandibular first premolar
3. Accessory canals are most frequently found in
A. The cervical one-third of the root
B. The middle one-third of the root
C. The apical one-third of the root
D. With equal frequency in all the above mentioned
4. A divided pulp canal is most likely to occur in the:
A. Root of a maxillary canine
B. Root of a mandibular canine
C. Root of a maxillary central incisor
D. Lingual root of a maxillary first molar
5. Mandibular first molar has:
A. 2 roots and 2 canals
B. 2 roots and 3 canals
C. 3 roots and 3 canals
D. 3 roots and 4 canals
6. Incidence of third root in upper first premolar
A. 6%
B. 10%
C. 12%
D. 1%
7. Pulp chamber is stained by:
A. 1% Methylene blue dye
B. 95% Ethanol and 17% EDTA
C. 1% Toluidine blue
D. Both A and B
8. Identify the Vertucci type:
A. Type 4
B. Type 5
C. Type 6
D. Type 3
9. Tooth that shows all type of Vertucci classification is:
A. Maxillary first premolar
B. Maxillary second premolar
C. Maxillary first molar
D. Mandibular second molar
10. Identify the isthmus type:
A. Type 2
B. Type 3
C. Type 1
D. Type 5
11. The point where pulp tissue ends and periodontal tissue begins is:
A. Cementodentinal junction (CDJ)
B. Apical constriction
C. Apical foramen
D. 3 mm from the apical foramen
12. Tooth that shows least size of main apical foramina:
A. Mandibular incisor
B. Maxillary premolars
C. Distal root of mandibular molars
D. Maxillary incisors
13. Tooth which does not obey first law of symmetry
A. Maxillary molars
B. Mandibular molars
C. Mandibular incisors
D. Mandibular molars
14. Buccal access if for (PGI JUNE 2015 question):
A. Crowded teeth
B. Rotated teeth
C. Lingually inclined teeth
D. Tooth with recession
15. C-shaped canal most commonly seen in:
A. Mandibular first molars
B. Mandibular second molars
C. Maxillary second molars
D. Maxillary first molars
16. Type 2 C-shaped canal is:
A. The shape is an uninterrupted “C” with no separation or division
B. The canal shape resembles a semicolon resulting from a discontinuation of the “C” outline, but either angle alpha or beta should be no less than 60 degrees
C. Two or three separate canals and both angles, alpha and beta, are less than 60 degrees.
D. Only one round or oval canal is in the cross-section
17. In anterior teeth, the starting location for access cavity is the center of the anatomic crown on lingual surface at:
A. Angle to it
B. In line to it
C. Perpendicular to it
D. All of the above
18. Most common chances of pulpal exposure will be there if pulpal floor is made perpendicular to the long axis of which tooth?
A. Maxillary first premolar
B. Maxillary first molar
C. Mandibular first premolar
D. Mandibular second premolar
19. Identify the tooth apex:
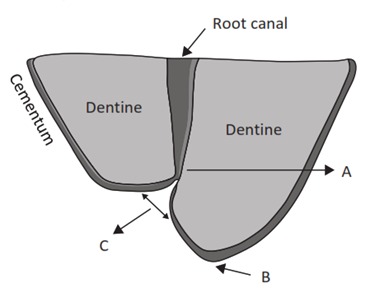
A. (A)
B. (B)
C. (C)
D. None
20. Percentage of distal root with two root canals in mandibular molar:
A. 10%
B. 30%
C. 60%
D. 1%
21. Morning glory appearance is present in
A. Floor of pulp chamber
B. Between minor and major apical diameter
C. Between walls of root canal
D. Tooth root apex and alveolar bone
22. What percentage of mandibular first molars have two distal canals?
A. 10 %
B. 30 %
C. 60 %
D. 75 %
23. Two canals are most often seen in the:
A. Maxillary canine.
B. Mandibular canine
C. Maxillary lateral incisors
D. Mandibular first molar
24. The fourth root canal if present in a maxillary first molar is usually present in:
A. Mesiolingual root
B. Mesiobuccal root
C. Palatal root
D. Distal root
25. The mandibular molars generally have:
A. Two roots and two canals
B. Two roots and three canals
C. Three roots and two canals
D. None of above
26. There are sharp demarcations between pulpal chambers and pulp canals in which of the following teeth?
A. Mandibular second premolars
B. Maxillary first premolars
C. Maxillary Lateral incisor
D. Mandibular canine
27. In the mandibular arch, the greatest lingual inclination of the crown from its root is seen in the permanent:
A. Canine
B. Third Molar
C. First premolar
D. Central incisor
28. The Mesiolingual root canal of the mandibular 1st molar is found under the:
A. Mesio lingual Cusp
B. Mesio Buccal Cusp
C. Central groove
D. Mesio lingual Ridge.
29. The orifice of the 4th canal in the maxillary molar is usually found:
A. under the Distofacial cusp
B. Lingual to the orifice of the Mesiofacial canal
C. on a line running from the Distofacial orifice to the Mesiofacial orifice
D. on a line running from the lingual orifice to the Distofacial orifice
30. If the Pulp of the single rooted canal is triangular and cross-section with the base of the triangle located facially and the Apex located lingually with the mesial arm longer than the distal the tooth is most likely:
A. Maxillary central incisor
B. Maxillary second premolar
C. Mandibular lateral incisor
D. Mandibular central incisor
31. Considering the morphology of root and pulp canals, a root canal instrument should be placed in what direction to gain access to the mesiofacial root of a permanent maxillary first molar?
A. From the Mesiobuccal
B. From the Distobuccal
C. From the Mesiolingual
D. From the Distolingual
32. In which anterior tooth has bifurcated roots presents:
A. Mandibular Lateral incisor
B. Maxillary Canine
C. Mandibular Central incisor
D. Mandibular premolar
33. Which of the following has the largest relative mesiodistal dimension of the root canal?
A. Maxillary Lateral incisor
B. Mandibular Second premolar
C. Palatal Root of the Maxillary 1st Molar
D. Distal Root of the Mandibular 1st Molar
34. Which root canal is most difficult to prepare in maxillary molar?
A. Mesiobuccal
B. Distobuccal
C. Palatal
D. Both A and B
35. The tooth most commonly having bifurcated roots is the:
A. Maxillary Central Incisor
B. Mandibular Lateral Incisor
C. Mandibular Central Incisor
D. Mandibular Premolar
36. The most easily perforated tooth with a slight mesial or distal angulation of bur after a Mandibular Central Incisor is :
A. Maxillary Premolar
B. Maxillary molar
C. Mandibular Premolar
D. Maxillary canine
37. A cross-section of the cervical third of the pulp canal of the maxillary second premolar resemble in shape:
A. A circle
B. A square
C. A triangle
D. An ellipse
38. Four canals are seen in:
A. Upper 1st molar
B. Upper 2st molar
C. Lower 1st molar
D. Lower 2st molar
39. The root canals most likely to share a common apical opening are:
A. Mesial and distal roots of mandibular premolars
B. Mesiobuccal and mesiolingual roots of mandibular first molar
C. Both A and B
D. None of above
40. Branching of pulpal canals is least likely seen in:
A. Maxillary central incisor
B. Upper 1st premolar
C. Mandibular central incisor
D. Mandibular lateral incisor
41. The anterior tooth most likely to display two canals is:
A. Maxillary Central
B. Maxillary Lateral
C. Mandibular Central
D. Mandibular Lateral
42. The tooth which usually has the largest pulp chamber in the mouth is :
A. Maxillary Central
B. Maxillary Canine
C. Maxillary 1st molar
D. Mandibular 1st molar